What is our current understanding of COVID-19? A gigantic and possibly never-ending question. It may appear that there is current COVID stability, but this is illusory, as new pathogenetic strains precipitating further pandemics are inevitable.
What about the demand for booster innoculations? Anti-COVID neutralising antibodies and clinical immunity produced by vaccines against SARS-CoV-2 virus are known to wane over a period of months.1 Antibody levels one booster dose after the primary series of vaccinations are fully restored but this effect also progressively declines. Fortunately, the 3-dose regimen including RNA-based vaccines is also highly effective against severe disease and death from the Omicron strain. The question arises as to whether a fourth dose will be required because of waning immunity, whether it will also be as effective as the initial “booster”, and if so will its effect also be transient? The underlying implication is that a regular programme of boosters may be required for control of COVID, even if there is no further mutation becoming the dominant strain, which is unlikely. This in turn raises the possibility of chronic restrictions on mobility and social interactions based on vaccine status, an issue raised in previous TMJ blogs. The European Medicines Agency and European Centre for Disease Prevention and Control have recently advised2 that though a second booster (4th vaccination) restores faded immunoglubulin levels and cellular immunity against COVID3 it does not have a major impact on disease incidence. The Agencies advised against a second booster for the general population but advised its use in high risk groups. A further background issue is whether infection with COVID produces immunity that is comparable to the immunity imparted by vaccination. The answer to that question raises issues related to the value of herd immunity (in its broadest sense) in overall disease control.
Natural immunity in COVID survivors is indeed protective against repeat infections. A study from Qatar4 reported substantial effectiveness against symptomatic infection and severe, critical or fatal Covid-19 infection for alpha, beta and delta strains, with lesser effectiveness against omicron for trivial but not severe infections. Study follow up was for 7 months. Effectiveness was defined as the “proportional reduction in susceptibility to infection among persons who had recovered from infection as compared with those who had not been infected.” Results are extracted in the table.
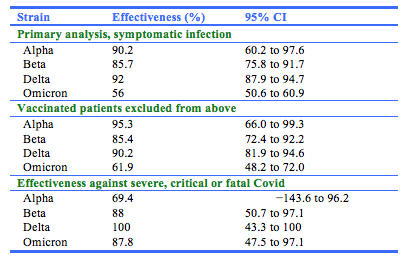
These data were generated for “previously infected patients” (that is, a positive PCR test found at least 90 days before a new positive PCR), compared to those having a negative test, presumably with the same delay (unfortunately, the study methods are not described in detail). These data are puzzling because it is known that IgG levels wane after natural COVID infection as well as after vaccinations, and in addition that antibody neutralisation is decreased with omicron.5 It is likely that T-cell immunity is also stimulated.6 In addition, when booster doses of vaccine are used, the process of “affinity maturation” of antibodies may come into play.7
The current situation in most developed countries is of ongoing new infections, facile spread of the omicron strain but with only moderately severe disease and reduced but still remaining risk of hospitalization, admission to ICU facilities, and death. These improvements are due to high vaccination rates and immunity from previous infections. Most demand for hospital services is in the unvaccinated, demonstrating the need for community accpetance of vaccine efficacy. Triple vaccination is required to achieve immunity against the omicron strain. Most governments of developed nations, with the notable interesting exception of China, have responded to the current epidemiology by lifting social restriction rules and have to date not reversed tack in the face of reflex increases in infection rates. It is to be hoped that the 2021 spike in mental illness caused by social dislocation will now decline, as people socialise and get back to work or school. There is now general tacit acceptance (except in China) that a “zero COVID” policy does not abolish infections and have a very high social and economic cost. These remarks apply to omicron; we await the next pathological COVID mutation with trepidation.
J A Millar
Editor, Tasman Medical Journal
References
- Andrews N, Stowe J, Kirsebom F, Toffa S, Sachdeva S et al. Effectiveness of BNT162b2 COVID-19 booster vaccine against covid-related symptoms and hospitalization in England. Nat Med https://doi.org/10.1038/d41591-022-00013-3 (2022)
- European centre for Disease Prevention and Control/European Medicines Agency. COVID-19: Joint Statement on the administration of a fourth dose of mRNA vaccines. https://www.ema.europa.eu/en/documents/public-statement/covid-19-joint-statement-ecdc-ema-administration-fourth-dose-mrna-vaccines_.pdf
- Munro APS Feng S Janani L et al. Safety, immunogenicity, and reactogenicity of BNT162b2 and mRNA-1273 COVID-19 vaccines given as fourth-dose boosters following two doses of ChAdOx1 nCoV-19 or BNT162b2 and a third dose of BNT162b2 (COV-BOOST): a multicentre, blinded, phase 2, randomised trial. Lancet Infect Dis. 2022 (published online May 9.). https://doi.org/10.1016/S1473-3099(22)00271-7
- Altarawneh HN, Hasan M, Ayoub HH, Qassim S, Almukdad S et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. https://www.nejm.org
- Planas D, Saunders N, Maes P, Guivel-Benhassine F, Planchais C. Considerable escape of SARS-CoV-2 Omicron to antibody neutralisation. Nature https://doi.org/10.1038/d41586-021-03827-2 (2021).
- Romero-Olmedo AJ, Schulz AR, Hochstätter S, Gupta DD, Hirseland H. Dynamics of humoral and T-cell immunity after three BNT162b2 vaccinations in adults older than 80 years. Lancet Inf Dis DOI: https://doi.org/10.1016/S1473-3099(22)00219-5.
- Gaebler C, Wang Z, Lorenzi JCCC, Muecksch F, Finkin S et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021; 591: 639–644 https://doi.org/10.1038/s41586-021-03207-w